
Waldenstrom’s macroglobulinemia is a rare form of lymphoma that occurs most often in older people. The disease is found in 3 people per million. If diagnosed in time, it has a good prognosis for treatment. Many patients live 14-16 years or more after diagnosis, provided therapy is started early.
Read about the symptoms, diagnosis, treatment and prognosis of Waldenstrom’s disease in our article.
Listen to the article:
Symptoms and signs of Waldenstrom’s Macroglobulinemia
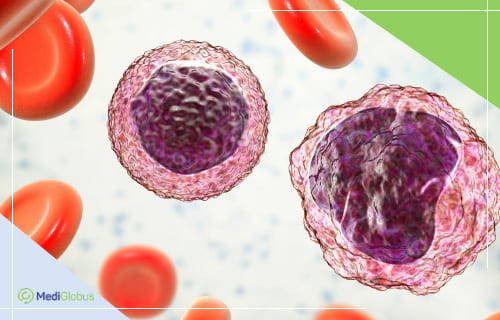
Waldenstrom’s macroglobulinemia is a rare type of non-Hodgkin’s lymphoma, a malignant disease of the bone marrow. In this disease, so-called lymphoplasmacytic cells are produced instead of healthy white blood cells. These are unable to perform a protective function and eventually accumulate in the body, replacing the normal cells in the bone marrow. This causes a general weakening of the body and several symptoms associated with macroglobulinemia:
![]() Weakness and fatigue;
Weakness and fatigue;
![]() Shortness of breath;
Shortness of breath;
![]() Weight loss;;
Weight loss;;
![]() Bruising;
Bruising;
![]() Bleeding from nose and gums;
Bleeding from nose and gums;
![]() Fever;
Fever;
![]() Migraines and headache;
Migraines and headache;
![]() Dizziness;
Dizziness;
![]() Blurred vision;
Blurred vision;
![]() Numbness in hands and feet;
Numbness in hands and feet;
![]() Painful sensitivity to cold.
Painful sensitivity to cold.
Abnormal lymphoplasmacytic cells continue to try to produce antibodies, just like healthy white blood cells do. However, instead, they secrete an abnormal protein – immunoglobulin IgM. It causes some of the symptoms characteristic of Waldenstrom syndrome. Large amounts of IgM cause blood clotting and interfere with the flow of blood through small blood vessels. They can rupture, causing bleeding in the nose, gums or retina. The protein also has a damaging effect on neurons.
Other signs that occur in the later stages of Waldenstrom’s macroglobulinemia include:
![]() Enlargement of the liver, spleen or lymph nodes due to an accumulation of lymphoplasmacytic cells;
Enlargement of the liver, spleen or lymph nodes due to an accumulation of lymphoplasmacytic cells;
![]() Amyloidosis of the heart and kidneys causes systemic dysfunction and may cause other diseases to develop.
Amyloidosis of the heart and kidneys causes systemic dysfunction and may cause other diseases to develop.
Waldenstrom’s macroglobulinemia is a slowly progressive disease. It can develop over several years without any symptoms.
Risk factors that increase the likelihood of developing the disease include:
![]() Age 65 and more;
Age 65 and more;
![]() Gender – males are twice as likely to have macroglobulinemia;
Gender – males are twice as likely to have macroglobulinemia;
![]() Heredity – having relatives who have had B-cell lymphomas.
Heredity – having relatives who have had B-cell lymphomas.
SIGN UP FOR A CONSULTATION WITH AN ONCOLOGIST
An experienced oncologist will help you to get a diagnosis and individualised treatment in a very short time. To book a consultation, please leave a request online. We will help you to find a doctor and conveniently conduct a consultation – in person or remotely.
What tests should be taken to diagnose Waldenstrom’s Macroglobulinemia?
Waldenstrom’s macroglobulinemia is rare in the population, so there are no standard diagnostic protocols as with other cancers. Usually, when a patient comes to a doctor with symptoms of the disease, he or she will be given a package of tests that can detect the presence of a malignant process. In many patients, macroglobulinemia is diagnosed accidentally during check-ups or examinations for other diseases.
To confirm the diagnosis, several tests are usually needed to pinpoint the cause of the ailment:
Blood test | In Waldenström syndrome, blood tests will show low levels of blood cells and high levels of IgM immunoglobulin. To monitor all organs, the blood test package usually includes the following tests: blood cell count, immunoglobulin levels, electrophoresis, blood viscosity test, cryocrit, cold agglutinins, beta-2 microglobulin (β2M). |
Bone marrow biopsy with aspiration | During the biopsy, the doctor uses a needle to remove a piece of bone marrow from the hip bone. The resulting tissue is sent to the laboratory to be examined for the presence of cancer cells. If these are found, advanced laboratory analysis is carried out to examine their characteristics, including genetic mutations. For a diagnosis of Waldenstrom’s disease, at least 10% of the cells in the bone marrow must have been replaced by lymphoplasmacytic cells. |
Visualization tests | Imaging tests such as CT, MRI and PET-CT are needed to rule out other diseases that can cause similar symptoms. In addition, these methods are used to look for metastases and to examine internal organs affected by macroglobulinemia. |
Treatment for Waldenstrom’s disease
Asymptomatic Waldenstrom’s macroglobulinemia does not require immediate treatment. In this case, the patient is found to have an elevated IgM level in the blood without any accompanying symptoms. In this case, the person remains under the care of an oncologist and is re-tested every few months to monitor the condition. The primary stage of the disease can last for several years. Doctors do not recommend the use of chemotherapy to treat it, to avoid undesirable side effects from the drugs.
The treatment plan for Waldenstrom’s macroglobulinemia depends greatly on the condition of the patient. More than half of the people diagnosed with the disease are over the age of 70. They can only tolerate mild chemotherapy protocols. In addition, the rate of progression of the disease and the presence of comorbidities are taken into account.

Chemotherapy
Chemotherapy acts as the main treatment for Waldenstrom’s macroglobulinemia. These drugs enter the bloodstream and reach almost all parts of the body, destroying the malignant cells. Treatment is carried out in cycles over several weeks, with breaks for the body to recover. As the drugs are prone to causing side effects, doctors usually prescribe accompanying medication to eliminate them.
Targeted therapy
These are drugs with a selective effect on malignant cells. They cause fewer side effects than chemotherapy and increase the effectiveness of the latter. Targeted therapy in combination with chemotherapy is considered the most effective treatment for Waldenstrom syndrome. This method is also used for relapses.
Immunotherapy
This is a group of drugs that use the patient’s immune system to destroy cancer, “training” it to recognise and resist pathologic cells. Several groups of drugs are used in the West to treat the disease: monoclonal antibodies, cytokines and immunomodulatory agents. Immunotherapy can be used alone or in combination with other drugs as an initial treatment or to treat relapsed Waldenstrom’s macroglobulinemia.
Bone marrow transplants
Bone marrow transplantation is a last resort treatment used in severe cases of Waldenstrom macroglobulinemia that are not susceptible to conventional oncotherapy. Given the risks, this procedure is only performed on young patients. In the vast majority of cases, autologous bone marrow transplantation is used, in which the patient’s tissue gets transplanted. During preparation, an aggressive course of chemotherapy is administered to destroy all disease-causing cells in the bone marrow. This is followed by the administration of pre-selected and prepared stem cells, which will restore the immune system. During the first 2-6 weeks the body has no protection against infections, so the patient has to stay in a sterile ward and undergo preventive therapy.
Plasmapheresis does not treat the cause of the disease, but it is prescribed to relieve the symptoms of most patients with Waldenstrom’s disease. The procedure is performed to lower the levels of IgM in the blood. A drip is injected into the patient’s vein, connected to a special machine. It ‘filters’ the patient’s blood, removing harmful proteins and leaving the necessary ones behind. The procedure takes several hours and does not require hospitalization. In cases where plasmapheresis will need to be carried out frequently, the patient may have a catheter inserted in the subclavian vein. In cases of severe macroglobulinaemia, transfusion of red blood cells and/or platelets may be necessary.
What is the prognosis for Waldenstrom’s macroglobulinemia?

Unlike most cancers, Waldenstrom’s macroglobulinemia is not divided into stages. The degree to which the disease has spread through the body has little effect on the prognosis and treatment of the disease. Instead, the International Prognostic Scoring System for Waldenstrom macroglobulinemia (ISSWM) is used. It takes into account other factors based on which the disease is divided into three subtypes: low risk, medium risk and high risk. A more positive prognosis is seen under these conditions:
![]() Patients under 65 years of age;
Patients under 65 years of age;
![]() Haemoglobin level higher than 11.5 g/dL;
Haemoglobin level higher than 11.5 g/dL;
![]() Platelet level – 100,000/mcL or higher;
Platelet level – 100,000/mcL or higher;
![]() Beta-2 microglobulin (β2M) level less than 3 mg/l;
Beta-2 microglobulin (β2M) level less than 3 mg/l;
![]() IgM level less than 7 g/dL.
IgM level less than 7 g/dL.
Depending on these indicators, the prognosis of patients with Waldenstrom’s macroglobulinemia is as follows:
| Risk level | Five-year survival rate |
|---|---|
| Low risk | 87% |
| Medium risk | 68% |
| High risk | 36% |
Most patients treated for Waldenstrom’s macroglobulinemia according to modern protocols live 14-16 years after diagnosis. Given that more than half of patients are over 70 years old when the disease is detected, their life expectancy is not much different from the statistical average.
A non-hereditary mutation in the CXCR4 gene is found in 30-40% of patients with Waldenstrom macroglobulinemia. It is associated with a more difficult prognosis.
Leading clinics for the treatment of Waldenström syndrome






Resume
![]() Waldenstrom’s macroglobulinemia is a type of non-Hodgkin’s lymphoma characterised by impaired B-lymphocyte production and elevated levels of IgM protein.
Waldenstrom’s macroglobulinemia is a type of non-Hodgkin’s lymphoma characterised by impaired B-lymphocyte production and elevated levels of IgM protein.
![]() To confirm the diagnosis, in addition to a blood test, a bone marrow biopsy should be performed. The analysis should show that more than 10% of the organ has been replaced by abnormal lymphoplasmacytic cells. Imaging tests are also usually prescribed: CT, MRI, PET-CT.
To confirm the diagnosis, in addition to a blood test, a bone marrow biopsy should be performed. The analysis should show that more than 10% of the organ has been replaced by abnormal lymphoplasmacytic cells. Imaging tests are also usually prescribed: CT, MRI, PET-CT.
![]() The treatment plan for Waldenstrom’s macroglobulinemia depends on the severity of the patient’s symptoms, age and state of health. The main treatments are chemotherapy, targeted therapy and immunotherapy. The drugs are chosen individually, depending on the patient’s tolerance. Plasmapheresis and/or blood cell transfusions may be used to relieve symptoms.
The treatment plan for Waldenstrom’s macroglobulinemia depends on the severity of the patient’s symptoms, age and state of health. The main treatments are chemotherapy, targeted therapy and immunotherapy. The drugs are chosen individually, depending on the patient’s tolerance. Plasmapheresis and/or blood cell transfusions may be used to relieve symptoms.
![]() In rare cases, young patients with Waldenström syndrome may receive an autologous bone marrow transplant.
In rare cases, young patients with Waldenström syndrome may receive an autologous bone marrow transplant.
![]() Alternative therapies such as immunotherapy, particularly CAR-T therapy, are gaining popularity. It is most often used when conventional therapies have failed. BiTE is another promising immunotherapy option that is being tested.
Alternative therapies such as immunotherapy, particularly CAR-T therapy, are gaining popularity. It is most often used when conventional therapies have failed. BiTE is another promising immunotherapy option that is being tested.
![]() The prognosis for the treatment of Waldenstrom’s disease is optimistic. Most patients are diagnosed with the disease at low risk, with a survival rate of 87%.
The prognosis for the treatment of Waldenstrom’s disease is optimistic. Most patients are diagnosed with the disease at low risk, with a survival rate of 87%.
![]() Clinics with extensive experience in treating non-Hodgkin’s lymphoma are located in Turkey, Germany, Austria, Spain, Israel and South Korea. Liv Ankara, the University Hospital of Navarra, the University Hospital of Cologne, the Ichilov Medical Centre and SoonChonHyang Hospital are popular among international patients.
Clinics with extensive experience in treating non-Hodgkin’s lymphoma are located in Turkey, Germany, Austria, Spain, Israel and South Korea. Liv Ankara, the University Hospital of Navarra, the University Hospital of Cologne, the Ichilov Medical Centre and SoonChonHyang Hospital are popular among international patients.
Sources:
- 1. National Organisation for Rare Disorders (NORD)
- 2. National Library of Medicine (NIH)
- 3. International Waldenstrom Macroglobulinemia Foundation (IWMF)
- 4. Leukemia: How to manage Waldenstrom’s macroglobulinemia
TREATMENT for Waldenstrom’s Macroglobulinemia
To book an appointment for treatment for Waldenstrom macroglobulinemia abroad, click on the button below and fill in the form. Our coordinators will call you back within 30 minutes. They will provide all necessary information and help with travel arrangements.
1.
2.
3.
4.

{kind=link}