
1. Causes of spinal metastases |
2. Diagnostics |
3. Methods of treatment |
4. Prognosis of survival |
5. Leading clinics |
About 30% of all stage 4 cancer patients have metastases to the spine – secondary foci of malignant lesions. They are caused by a tumour that originally appeared in another organ. Spinal metastases affect men more often than women. Most cases occur between the ages of 40 and 65. Treatment options for the disease vary from case to case. Read this article to learn how spinal metastases are treated abroad and what results can be achieved.
Listen to the article:
When do spinal metastases appear?
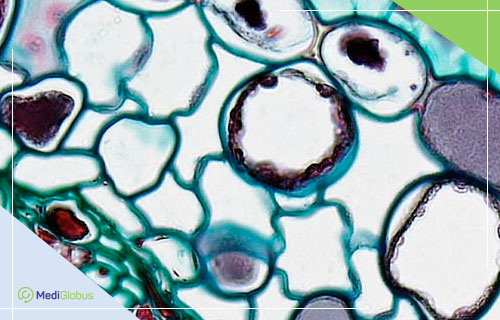
Various types of cancer can spread to the spine. This is an indication that the malignancy has progressed to an advanced stage. The cancer cells of the primary neoplasm “migrate” through the body with the blood and settle in the spongy substance located in the vertebral body.
Spine metastases account for about 90% of all cancers in this area. This is one of the most common types of secondary tumours. Lung and liver metastases come first and second.
Malignant neoplasms of internal organs can metastasise to the spinal column. These are at the top of the list.
These include lung, gastrointestinal, uterine, ovarian, bladder and kidney cancers. It is also common for cancer of the prostate, breast, trachea, tongue and larynx to metastasise to the spine. Many patients with advanced melanoma or multiple myeloma have this type of secondary foci.
You can find out more about cancer metastasis to the spine by contacting our specialists. We arrange offline or online consultations with leading oncologists abroad.
What are the symptoms of spinal metastases?

Metastases to the spine impair its support function and can cause a host of neurological abnormalities. The clinical picture is determined by the extent of damage to the spinal column and the localisation of the secondary tumours. Approximately 70% of symptomatic lesions occur in the thoracic spine, slightly more than 20% in the lumbar spine, and about 10% in the cervical spine.
The main symptom of the disease is pain. It may be located not only in the back but also irradiate to the limbs or the pelvis. The nature of the pain depends on how much the tumour pushes on the spinal cord and nerve roots.
The larger the lesion, the more severe the symptoms. Patients usually complain of dull or aching pain in the spinal column.
Other signs of spinal metastases are:
![]() impaired motor activity,
impaired motor activity,
![]() memory impairment,
memory impairment,
![]() numbness or tingling in the limbs,
numbness or tingling in the limbs,
![]() paralysis and loss of sensation,
paralysis and loss of sensation,
![]() coordination disorders,
coordination disorders,
![]() muscle weakness,
muscle weakness,
![]() uncontrolled bowel movements or urination.
uncontrolled bowel movements or urination.
How are spinal metastases diagnosed?
Many patients ask if bone metastases can be seen on an X-ray. The answer is yes. The X-rays show specific and non-specific changes in the bone tissue, which may indicate the presence of a cancerous process. However, magnetic resonance imaging or computed tomography will provide more detailed information that will help to identify metastases in the spinal column.
Diagnosing a metastatic lesion in the spine begins with a physical examination. This allows signs of spinal cord compression to be detected. The patient is then given a CT, MRI or PET-CT scan. These examinations also make it possible to assess the degree of spinal cord compression.
The appearance of spinal metastases on CT and MRI scans will depend on the level of mineralisation of the cancer cells. The most common are lytic secondary tumour foci. They appear as areas of soft tissue loosening with jagged edges.
You can book an appointment for an oncological diagnosis at one of the leading clinics abroad by leaving an application form on the MediGlobus. We will help you with organising your medical trip in the shortest possible time.
Can spinal metastases be cured?
Treatment of vertebral metastases depends on the severity of the pathology and the type of primary tumour. Controlling secondary lesions does not cure cancer by itself. It is aimed at reducing the size of the tumour and slowing down or stopping its growth. Also, treatment of metastatic lesions helps to preserve the stability of the musculoskeletal system and alleviate pain or neurological symptoms.
Spinal metastases are predominantly treated with surgery, radiation, and chemotherapy and complemented by painkillers. These methods of dealing with the disease are combined and rarely used in isolation.
The goal of surgical intervention for metastases is to achieve nerve decompression with simultaneous reconstruction and immediate stabilisation of the vertebral column. This is possible through the use of various surgical approaches and multiple vertebral fixation devices.
Removal of spinal metastases can be done minimally invasively (through small punctures or incisions) or openly. The types of minimally invasive surgeries used for this disease are:
Laparoscopic laminectomy – removal of the vertebral arch affected by a tumour. The operation is recommended to relieve nerve compression and remove abnormal tissue. The surgery lasts 1-3 hours and involves general anaesthesia.
Vertebroplasty is the removal of metastases using a special needle and microsurgical instruments. The bony defect is filled with special cement. This stabilises the spine, exacerbates pain and restores its functionality.
Kyphoplasty is the removal of a cancerous lesion, followed by correction of the shape of the vertebrae. The procedure involves inserting a special tube with a balloon at the end into the affected area of the spine. The balloon is then inflated to reshape the vertebra. To preserve the result, the spine is fixed with bone cement or titanium plates.
In cases of spinal metastases, open surgery is avoided. This is because such a technique involves a large incision and more tissue trauma. The potential benefits may not be worth the risks.
Elderly patients and people with many comorbidities may not be able to tolerate surgery. Patients with critically advanced pathology are also contraindicated, as surgery makes little difference in the life expectancy.
If the metastases are without spinal cord involvement and the person has no significant symptoms, conservative treatment is indicated. This includes pain medication and steroids along with chemotherapy and/or radiation therapy. CyberKnife radiosurgery may be an option.
Transarterial chemoembolization is recommended for multiple spinal lesions. The procedure involves injecting an anti-tumour “blocking” agent directly into the vessel that feeds the neoplasm. This reduces or destroys the metastases and relieves pressure on the nerve roots or spinal cord.

Specific treatments for spinal metastases
Given the fact that the choice of treatment depends directly on the primary tumour, doctors may use standard methods as well as more specific ones.
For example, some cancers, such as multiple myeloma, small cell lung cancer and lymphoma, respond better to radiation therapy than to surgery. It is therefore the number one choice when these tumours have metastasised to the spine.
Targeted or immune medications are also used in these cases. They target both the primary tumour and the secondary tumour.
Metastases in breast and prostate cancer respond well to hormonal therapy, with even greater emphasis on chemotherapy. Xofigo or Lutetium are recommended for those patients.
Patients with advanced inoperable prostate cancer may be prescribed Xofigo. This is a medicine containing the radioactive substance Radium-223 dichloride. It is administered intravenously, under the supervision of radiation specialists. It identifies the cancer cells and destroys them with powerful alpha radiation.
The number of sessions and the dosage are calculated individually for each patient. Usually, 1 to 6 injections are enough to get the maximum effect. The minimum interval between injections is about one month.
Lutetium is a worthy alternative to chemotherapy for metastatic prostate cancer and neuroendocrine tumours (gastric, pancreatic, thyroid oncology, etc.). The drug consists of the isotope Lutetium-177. This substance recognizes protein receptors on the surface of cancer cells and destroys them. Lutetium is administered intravenously. Usually, 3-4 sessions are needed at 4-5 week intervals.
What is the survival rate for spinal metastases?
Many forums state that the prognosis for spinal metastases is unfavourable. However, the earlier a patient seeks medical help, the better the chances of survival. The prognosis is also influenced by the type of primary neoplasm. For example, the 5-year survival rate for lung cancer patients with metastases to the spine is 4-15%, but for patients with advanced breast cancer, it is about 22%.
The survival rate for spine metastases varies on average from 3 to 10 months. This figure applies to advanced and inoperable cancers. Patients who undergo surgery in conjunction with other oncotherapy options can achieve a life expectancy of 3 years, and sometimes longer.
Where are spinal metastases treated abroad?






Resume
![]() Approximately 90% of all malignant neoplasms of the spine are thought to be metastatic in origin. This is one of the most common places where different types of cancer progress. Lung, breast, kidney, GI tract, bladder, prostate, throat, trachea and tongue cancers are most likely to metastasise into the spine.
Approximately 90% of all malignant neoplasms of the spine are thought to be metastatic in origin. This is one of the most common places where different types of cancer progress. Lung, breast, kidney, GI tract, bladder, prostate, throat, trachea and tongue cancers are most likely to metastasise into the spine.
![]() The clinical presentation of metastatic lesions of the spinal column depends on the localisation and degree of involvement. For example, sacrum metastases have symptoms such as radicular sensitivity disturbance, dull or aching pain in the lower back, numbness in the lower extremities, etc.
The clinical presentation of metastatic lesions of the spinal column depends on the localisation and degree of involvement. For example, sacrum metastases have symptoms such as radicular sensitivity disturbance, dull or aching pain in the lower back, numbness in the lower extremities, etc.
![]() Spinal metastases can be seen on CT, MRI, PET-CT or X-ray. The first three diagnostic options are more informative.
Spinal metastases can be seen on CT, MRI, PET-CT or X-ray. The first three diagnostic options are more informative.
![]() Vertebral metastases are treated based on the primary tumour. Accordingly, in addition to standard therapy options (surgery, chemo, radiosurgery, radiation), more specific methods of control are available in some cases, such as Xofigo for prostate cancer or Lutetium for gastric, pancreatic and prostate cancer.
Vertebral metastases are treated based on the primary tumour. Accordingly, in addition to standard therapy options (surgery, chemo, radiosurgery, radiation), more specific methods of control are available in some cases, such as Xofigo for prostate cancer or Lutetium for gastric, pancreatic and prostate cancer.
![]() The prognosis for spinal metastases depends on the severity of the disease. The average survival rate for complicated cases is 3-10 months. With timely treatment, the patient can live for 3 years or even longer.
The prognosis for spinal metastases depends on the severity of the disease. The average survival rate for complicated cases is 3-10 months. With timely treatment, the patient can live for 3 years or even longer.
![]() For spinal metastatic lesions, patients prefer clinics in Turkey, Spain, Israel and South Korea. These include the American Hospital in Istanbul, Koç, Liv, Assuta, Teknon and SNUH.
For spinal metastatic lesions, patients prefer clinics in Turkey, Spain, Israel and South Korea. These include the American Hospital in Istanbul, Koç, Liv, Assuta, Teknon and SNUH.
To arrange treatment for spinal metastases abroad, click on the button below and fill in the feedback form. We will help you with the selection of a clinic and a competent doctor, as well as with all matters from preparation for the medical trip to the patient’s return home.

{kind=link}